
Our Courses
Provide a general summary of the services you provide, highlighting key features and benefits for potential clients.


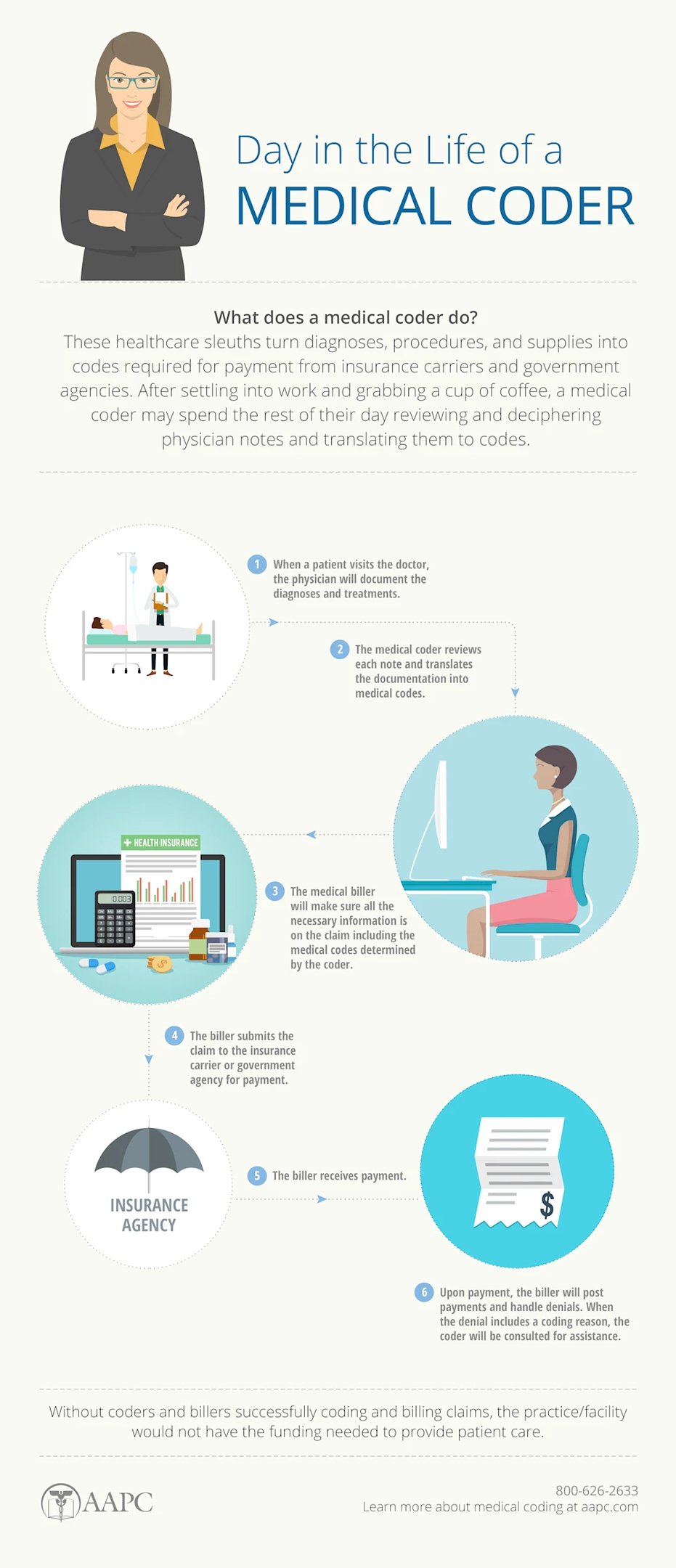
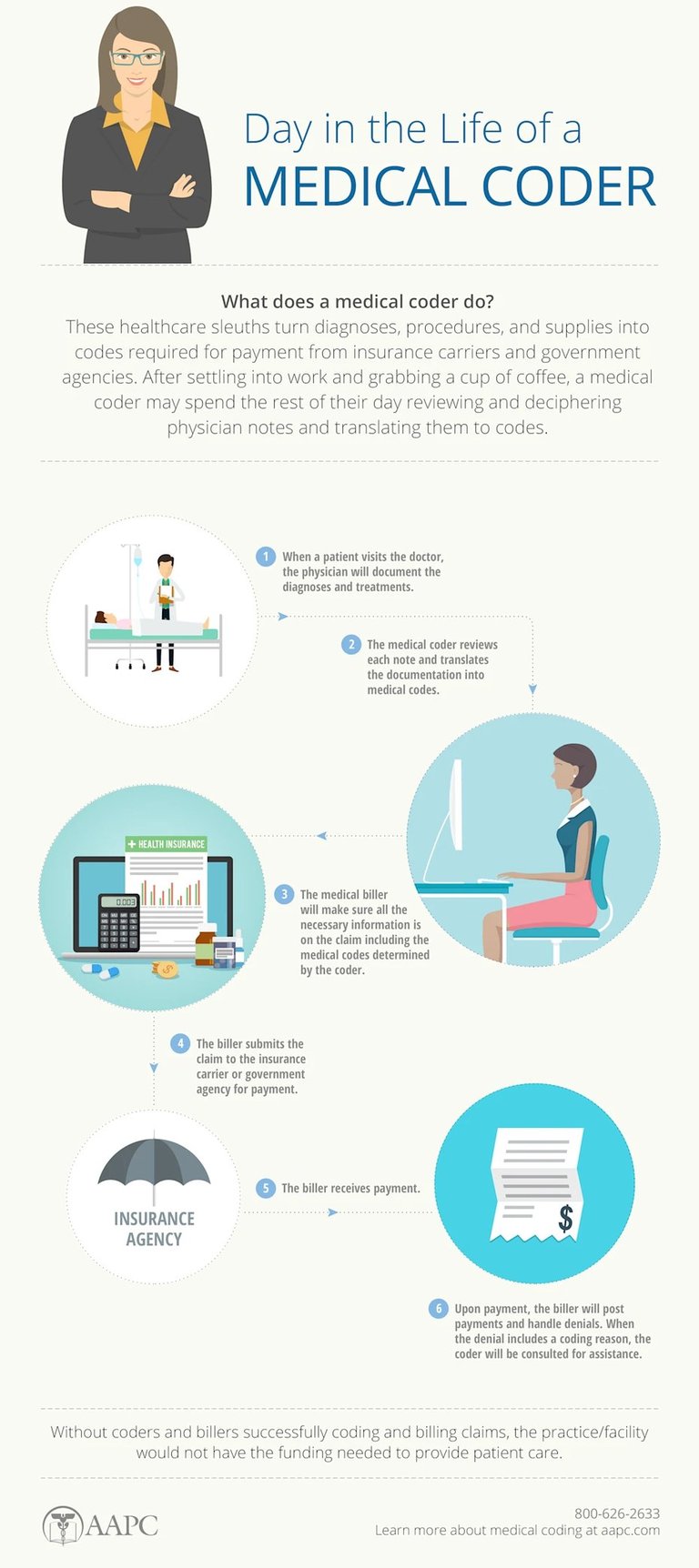
What is Medical Coding?
Medical coding is the transformation of healthcare diagnosis, procedures, medical services, and equipment into universal medical alphanumeric codes. The diagnoses and procedure codes are taken from medical record documentation, such as transcription of physician's notes, laboratory and radiologic results, etc.
Medical coding professionals help ensure the codes are applied correctly during the medical billing process, which includes abstracting the information from documentation, assigning the appropriate codes, and creating a claim to be paid by insurance carriers.
Medical coding happens almost every time you see a healthcare provider. The healthcare provider reviews your complaint and medical history, makes an expert assessment of what’s wrong and how to treat you, and documents your visit. That documentation is not only the patient’s ongoing record, it’s how the healthcare provider gets paid.
What you will learn?
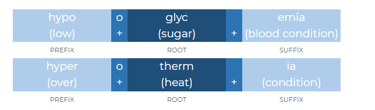
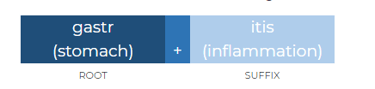
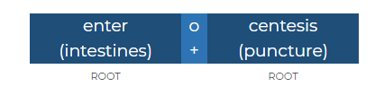
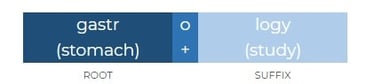
Medical Terminology
Human Anatomy & Physiology
Pathophysiology
About Course
Medical coders translate documentation into standardized codes that tell payers the following:
Patient's diagnosis
Medical necessity for treatments, services, or supplies the patient received
Treatments, services, and supplies provided to the patient
Any unusual circumstances or medical condition that affected those treatments and services
Medical Coding









Quick links
Contact Us
+91 - 80720 20716
medicalcodingofficers@gmail.com
All Rights Reserved. Website Design by Medical Coding Officers Academy
Medical Coding Officers Academy
India's top most training center for medical coding, billing and RCM in healthcare industry.
Subscribe to our newsletter
70/1, 2nd Floor, 200 Feet Radial Road, Pallavaram to Thuraipakkam Road, Near A2B Restaurant, Pallikaranai, Chennai, Tamil Nadu 600100